Breast Augmentation
(In Male-to-Female transsexuals)

| Introduction |
The breasts are a very visible and important aspect of every transsexual woman's "womanhood" and beauty - indeed such is the importance of breasts that breast augmentation is often the first surgery that she has.
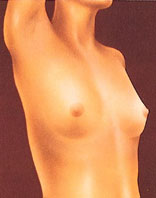
Female hormone treatment alone often results in insufficient
growth of the breast. If the woman is already past puberty when she starts treatment, the resulting breast development can range from satisfactory to very disappointing - although even in the later case it should be remembered that modern bra's, "push-ups" (see a typical advert, right) and breast enhancers can still do wonders appearance wise and that breast augmentation should not be an automatic choice given the costs and risks always associated with any surgery.

A majority of transsexual women eventually seek augmentation mammoplasty (breast implants), 50-60% is commonly quoted in research papers. A Dutch study of 200 transsexual women found that they usually sought a distinctly "feminine figure" and that two-thirds had had breast augmentation - in some instances repeatedly if the initial augmentation had not been outspoken enough!
Good breast implants can dramatically improve the appearance, passability and attractiveness of a transsexual woman.
In some countries transsexual women form a non-trivial proportion of the total breast augmentation market. For example, according to the BAAPs, about 10,000 breast augmentation operations are undertaken in the UK per year. The NHS performs about 100 breast augmentations per year on male to female transsexuals, and a much larger number are privately funded. Perhaps 2-3% of all breast augmentations in the UK are performed on genetic men - predominantly transsexual women and shemale prostitutes, but also intersex women, drag artists, a few homosexuals and transvestites, and on at least one occasion a man just doing it to win a bet!
Disappointingly, despite the demand, very few surgeons cater properly for transsexual women and their special needs and desires, and those that do often charge excessively.
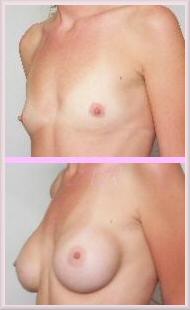
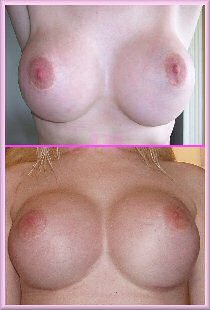
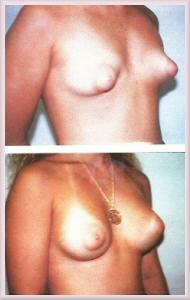
You get what you pay for ... whilst the transwoman on the right has clearly had implants, the appearance of her breasts is far superior to girl on the left, even though their implants are of similar size.
What is Breast Augmentation?
While it can vary over time and with fashions, the perfect breast will always be symmetrically balanced and proportionate to the rest of the body. Breast augmentation, technically known as augmentation mammoplasty, is a surgical procedure to enhance the size and shape of a woman's breast by inserting an implant behind each breast. The usual goal of breast augmentation is to achieve the most beautiful and natural looking breasts possible - although some women do not always desire a natural look!
The gorgeous Jamie Clayton had small breast implants to subtly enhance her hormone induced breast development. However in this picture the shape and outline of the implant in her right breast is obvious, and the exceptional distance between her breasts looks very odd.
To create an aesthetic and symmetrically balanced breast using implants to enhance them is not an easy task. However breast augmentation is a very well established and straightforward procedure that is capable of producing excellent results - it's certainly no secret that many top models and actresses have had breast augmentation.
Excessively large implants or poor quality surgery make the breast augmentation very obvious, indeed it is important to emphasise that breast augmentation is always detectable via scaring, shape, appearance, movement and/or feel. Good quality surgery, an appropriate implant size, and a well fitting bra will often result in a clothed appearance that (even with a low cut top) that is indistinguishable from any woman with natural breasts, and is totally passable. The very best augmentation results are hard to identify even when the transwoman is wearing a skimpy bikini top, however some problems are almost certain to become obvious visible if she then makes the next step of going topless. Unclothed, augmentation is impossible to hide from an intimate partner.
Three very pretty girls, but their breasts are obviously enhanced
by implants and they have the typical transsexual giveaway of small areola.
For best results in a transsexual woman, augmentation should not be undertaken before maximum breast development from hormone use has been achieved, the more breast tissue available the better. Rushing in to breast augmentation at the start of a transition and hormone treatment is a common but massive considerable mistake. Breast implants that have only skin coverage are likely to appear artificially round, with the edges of the implant plainly showing. As a rule of thumb, if the breast size is still unsatisfactory after two years of hormone therapy then augmentation becomes appropriate.
Caroline Cossey - formally Barry Cossey - has had at least eight breast augmentation operations since she transitioned in 1971 (left). Her famous Playboy magazine spread in 1991 - the first transsexual to be knowingly featured by the magazine - shows her with fairly natural appearing 36C breasts, albeit clearly augmented via the inframammary method.
Anyone considering breast augmentation must take in to account that it is a fairly significant surgical procedure and that complications often result (as shown below). Also breast implants have a finite life - typically they need replacing after 7-12 years. A transsexual woman choosing to have breast implants thus faces the cost and trauma of having replacement surgery every ten years or so for the rest of her life. The only slight positive is that recovery from a replacement procedure tends to be a shorter and less painful period than from the initial augmentation procedure.
This picture of Thai transsexual showgirl's (katoey's) shows a mixture of hormonal breast development and implants of varying quality. (Click to enlarge)
Additional chapters in This Section include:
Gender Reassignment Surgery
Orchiectomy for MTF Transsexual Women
FFS Facial Feminization Surgery
MTF Transsexual Surgeries
Hormone Replacement Therapy for Transgender Women
Female Hormone Therapy MTF Transsexuals
Breast Development in MTF Transsexuals
MTF Transsexual Breast Enlargement
Breast Augmentation MTF Transsexuals
Lactation and the Transsexual Woman
Injecting Silicone for Transsexual Women
Brazilian Hips and Buttock Enlargement
Average Body Size MTF Transgender
Male and Female Skeleton Transsexuals
Treatment of Young Transsexuals
Puberty in Adolescents MTF Transgender
Treatment of Young MTF Transsexuals
Treatment of Intersex Infants
Androgen Insensitivity Syndrome
Female Physical Beauty Transgender
Transgender Female Beauty
Exercise, Fitness and Diet for Transsexual Women
Breast Shape
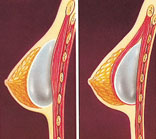
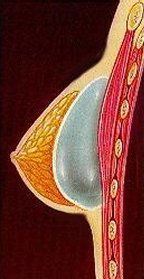
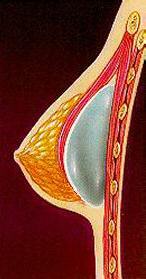
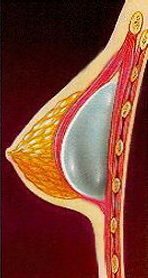
For an understanding of breast implants, it's important to first consider how a breast gets and maintains its shape.
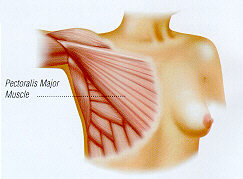
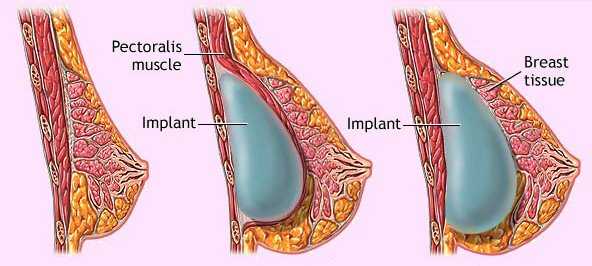
The female breast is made up of fatty, glandular and fibrous tissues. Within it are blood vessels, milk ducts, fat, glands and sensory nerves. A layer of fat surrounds the breast to give it a soft consistency and contour. Beneath the breast there is the pectoralis major, a large muscle that assists in arm movement.
The Breast consists of milk ducts and glands surrounded by fatty tissue, and covered by skin. The fatty tissue gives the breast its soft feel and shape. Skin elasticity also affects breast shape.
The pectoralis major muscle lies beneath the breast, and indirectly affects breast projection. The pectoralis major muscle helps with flexing and rotation of the arm at the shoulder joint.
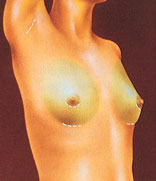
A good result but note the excessive gap between breasts, common in transsexual women. Small areola, even after augmentation, is another very common problem faced by transwomen.
Women's breasts vary greatly in both size and shape. The size of the breasts are determined by the amount of breast tissue and fat present in them. The actual shape of the breast is determined by the shape of the skin envelope, not by the shape of breast tissue within that envelope. The breast tissue acts as a "filler" which is shaped by the skin envelope; if it were removed from the envelope it has no shape of its own. Hence, the basic shape of a breast following augmentation will be similar, but with a fuller volume, than before the procedure. The shape is also affected by factors such as age, genetics and skin elasticity. The shape of the breasts of genetic women can also change dramatically as a result of pregnancy and breast-feeding. Even breasts on the same body can vary, one being slightly different from the other, such variations in size and shape are normal and they occur in most women.
Breast cleavage is infact produced by a bra. Very few breasts naturally point directly forward off the chest wall, the usual breast position being slightly "down and out" with little apparent cleavage. Without a bra, the upper profile of the breast in side view is usually straight, regardless of the size of the breast. Excessive outward bulging with an outwardly curving contour in the upper breast is a telltale sign of excessive augmentation.
The space between the breasts also varies widely from woman to woman, but it is generally on the large size for transsexual women due to their above average rib cage size combined with below average breast size.
Beautiful Breasts
It's Not All About Size
Most transsexual women tend to think only in terms of their bra cup size when considering their breasts and breast augmentation. For instance, if they're a 36A after hormone treatment, then their main concern may simply be becoming a 36C bra size after augmentation.
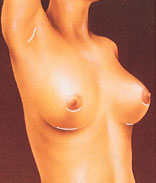
A very natural looking augmentation. Anatomical teardrop shaped implants were inserted through an inconspicuous incision under the armpit. A Genetic woman.
While doctors half-heartedly say that it is not all about size, many of their patients clearly disagree. Half of all breast augmentation patients want breasts over 600cc total volume. In the typical transsexual women this correlates to implants of roughly 400cc - a very substantial implant with no real prospect of a natural look.
Implants indeed add volume to the total breast tissue and the larger the desired cup size, the larger the volume (measured in "cc's") of the implant. However, breast augmentation is not just about bigger breasts; it's about shape and balance. The real goal of augmentation surgery is to have beautiful and attractive (sexy!) breasts.
Beautiful breasts come in all sizes cup size is not the only consideration. There should also be concerns about breast shape, proportions and overall body figure. There are many factors that are the basis for determining "beautiful" breasts.
Factors to Consider
Everyone woman has a different body shape which should influence the contours of the enhanced breast. Different breasts and body contours will determine the size and style of the implant and in some cases the location of the incision as well.
Slope
Aside from the size issue, a beautiful breast has several components. First, it is desirable to have a gentle slope that extends from just below the clavicle to the peak of the breast at the nipple position. A bulge in that region is a telltale sign of an implant and a "scooped-out" area probably means the breasts are too saggy. A smooth, gentle line should be present.
Nipple Position
Second, the nipple position should be in the region of the centre of the breast mound. The nipple should tilt slightly outward and upward. Then the line of the breast should dip in a gentle arc from the nipple to the breast fold.
Breast Width
Breast width is an especially important dimension, because it determines how much cleavage there is between the breasts. Breast width also determines the outside curve of the breasts, which helps balance the hips and narrow the waist.
Many transsexual women suffer from underdeveloped breasts but seek distinctly feminine breasts -- generally larger than most surgeons recommend. This girl was originally a 36A, the first surgery took her to a 36B/C (360cc) and the second to a 36DD (676cc). The result is unusually good and natural looking for such a large increase.
Cleavage
Cleavage is always desirable, and when the breast is viewed from the front in silhouette or from the back, there should be a gentle suggestion of fullness in the midline and laterally.
Size
Once all these components are considered, the overall breast size becomes the final factor. The optimum breast size is determined by measuring and studying the woman's body shape and bone structure. A good surgeon will ask the woman to pick pictures or photographs of breasts that she feels are desirable.
Two Points of View
Even after considering professional advice, the reality is that what many transsexual women desire and regard as "beautiful breasts" is not what their surgeon (or indeed a photographer of topless models) would regard as "beautiful breasts", or least the best and most natural looking achievable for the woman. For every girl seeking small implants (perhaps just 100cc) and hopefully almost undetectable implants to help fill out her breasts to at least a modest size for her build, there is another seeking large implants (over 500cc) and obviously unnatural looking breasts - Pamela Anderson in her heyday being an ideal.
One common problem is that all too often girls who have the least natural development, and thus are most unsuited for large implants, are the one's seeking the largest augmentation. To avoid unnecessary dissatisfaction and repeated surgery, the British Association of Plastic Surgeons sagely advises its members: "For a male-to-female transsexual patient to appreciate the outcome of augmentation mammoplasty, the surgeon should tolerate and address this patient's urge for a distinctly feminine breast configuration." Transsexual girls wanting very large implants (over 1000cc is not unusual) face great problems finding a reputable surgeon willing to perform the procedure.
Breast Augmentation Procedure
Different surgeons, depending upon their preferences and prior experiences, perform the breast augmentation procedure differently. Also, the method of inserting and positioning the implant will depend on the patients' anatomy and the desired size and shape of breast.
However, it would be reasonable to say that the following method is usually followed:
| The patient and surgeon agree on the desired size, shape and look of the augmented breast. |
| The type (smooth or textured), shape (round or anatomical) and size (measured in cc of volume) of implant is selected. The implant may contain saline, silicone gel, or some other filler. |
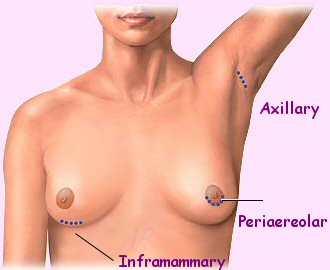
| The incision site is determined; this can be nipple (areolar), armpit (transaxillary), under the breast (inframammary) or navel (transumbilical). |
| The site of implant placement is decided; this can be above the muscle (subglandular) or below the muscle (submuscular). |
Breast augmentation by a transsexual women is usually undertaken in order provide the largest and most beautiful and natural looking breasts possible.
Incisions are made to keep scars as inconspicuous as possible, in the breast crease, around the nipple, or in the armpit. Breast tissue and skin is lifted to create a pocket for each implant.
The breast implant may either be inserted directly under the breast tissue just above the Pectoralis muscle (subglandular) or behind the pectoralis muscle and above the ribcage (submuscular).
After surgery, breasts appear fuller and more natural in tone and contour. Scars will fade with time.
Transwoman Kate after breast augmentation to a C-cup. Unfortunately the breasts are not symmetrical, and the cleavage looks slightly strange.
While breast augmentation will reliably make the breasts larger, it will not change the underlying basic shape of the breasts, a factor that may vary significantly from patient to patient. The shape of the breasts after implant enlargement or augmentation mammoplasty is mostly determined by the breast shape before surgery, the post-op augmented breasts will generally appear to be a larger version of the original breasts. A careful examination of the woman is thus very important since her physical characteristics will have a great bearing on the final shape of the enlarged breast. Factors determining the augmented breast appearance include the shape and symmetry of the ribcage and muscles, the shape and depth of the breastbone, the volume of the existing breasts, and the character of the existing breast skin. The position and symmetry of the existing breast folds and nipples, and the woman's height and weight also have a significant impact on the achievable appearance.

After surgery, breasts should appear fuller but natural in tone and contour. Scars will fade with time.
Some degree of breast asymmetry is normal, volume and size differences of the breasts often can be corrected by implant volume adjustments, for example as saline filler is added is added to saline implants. But often it is not possible to correct many of the asymmetries that are commonly seen, such as different heights of nipples or infra-mammary folds.
Types of Implant
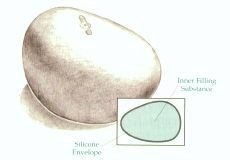
All breast implants have an outer pliable envelope enclosing either a liquid (usually saline) or soft-solid gel like substance (usually silicone gel). The surface of the implants has traditionally been smooth to the touch, but now there is another option, a textured surface.
To help meet each woman's individual needs, various sizes and shapes of implant are available. Some are specifically intended to benefit transsexuals with rather large upper-body proportions - most transsexual women have 'male-sized' rib-cages and tend to have their natural breasts located somewhat further apart than on a natural-born XX woman, this makes the breasts look subjectively smaller and lacking a well-defined cleavage. Shaped implants can remedy this situation by adjusting the shape of the breasts to produce a subjectively larger cleavage.
Material
A breast implant is actually a silicone elastomer shell - a rubber-like membrane or envelope. To achieve fullness and create the most natural breast-like feeling possible, this shell is filled with some suitable material - but finding a material that exactly but safely duplicates the feel and movement of breast tissue has been a long running challenge. Currently, the vast majority of implants are either silicone gel or saline filled; however some other fillings have recently appeared.
Silicone gel filled implants were the most common type for some 30 years, but have been avoided in the USA since the early 1990's due to unproven but suspicious health problems associated with the gel. Saline implants are considered to be totally safe and are now usually preferred, but unfortunately they give a less natural feel than silicone gel. Saline implants are currently (2001) the only type approved by the Food and Drug Administration for use in the USA, although silicone gel implants are still available in special circumstances. Other alternatives to silicone gel include hydrogel and plant oil filled implants have been recently developed, but their long term safety is still unproven, for example the UK's Medical Devices Agency advises against these fillings, recommending only silicone gel or saline implants.
Silicone Gel Filled Implants
These are bags of silicone gel, i.e. they are silicone gel (a soft-solid substance) inside a smooth or textured elastomer shell also made of silicone.
Silicone gel implants were first developed in the early 1960s after it was discovered that injections of silicone, which had previously been used for breast enlargement, could lead to unacceptable complications. Silicone gel has an excellent texture as a filling material because it is soft and pliable and allows for very natural breast feel and movement.
Subpectoral, periareolar, 310cc implants
Initially capsule contracture was a major problem with silicone gel implants, but the incidence rate is however much reduced with the latest implant types. Silicone implants do interfere with the standard mammography techniques, but this can usually be overcome by informing the radiologist about the presence of the implant so he or she can alter the technique to obtain the optimum result ("Eklund Distraction Technique").
Leakage or bleed of free silicone gel from the implant in to the breast, or elsewhere, may cause silicone granulomas to form. These are lumps of inflammatory tissue around small amounts of silicone. These lumps can often mimic the lumps which indicate breast cancer, but these silicone granulomas are not cancer and do not appear to increase the risk of cancer. There has been no evidence that silicone gel is related to connective tissue disease. In fact silicone appears to be one of the most inert materials known. However, the perceived - but not proven - safety concerns have stopped the unrestricted use of silicone gel implants in the USA, the Food and Drug Administration has restricted their use since April 1992. There is no sign of this ban being reversed despite many recent in-depth studies clearing silicone gel implants of any cancer risk, and the fact that many countries, including the United Kingdom, continue to permit their use.
An Independent Review Group sponsored by the UK Government undertook a detailed study of silicone gel breast implants in 1998-2000 and their findings concluded:
| There is no histopathological or conclusive immunological evidence for an abnormal immune response to silicone from breast implants in tissue. |
| There is no epidemiological evidence for any link between silicone gel breast implants and any established connective tissue disease. If there is a risk of connective tissue disease, it is too small to be quantified. The IRG cannot justify recommending further epidemiological studies to investigate this hypothesis. |
| Good evidence for the existence of atypical connective tissue disease or undefined conditions such as ‘silicone poisoning’ is lacking. It is possible that other conditions such as low grade chronic infection may account for some of the non-specific illnesses noted in some women with silicone gel breast implants. |
Saline Filled Implants
Saline-filled breast implants have been available since the late 1960s but they were largely viewed as an "alternative" breast implant in a market dominated by the popular gel-filled device. Saline filled implants have only become popular since 1992 when the FDA decided to restrict the use of silicone gel-filled breast implants, and they now dominate the market in the USA (though not elsewhere).
Saline filled implants are simply bags of water. The water is salt water, osmotically equal to the natural salt content of the body and completely harmless. The saline is contained within what's technically called a silicone elastomer shell. If the bag breaks, the body safely absorbs the saline that leaks.
Recently fixed-volume pre-filled saline implants have become available, but most saline implants are inserted uninflated and then filled when in place, before removing the valve and closing the incision. This technique has the significant advantage over silicone gel implants (which are always pre-filled) that the incision the implant is inserted through can be much smaller (typically 2-3cm, against 4-5cm). Also the surgeon can adjust the filling level for a best appearance, including adding different amounts to the two implants to help correct any breast size difference.
Most surgeons and patients are of the opinion that silicone gel implants have a more breast like feel when compared with saline filled implants, which feel a little "watery" and firmer, and fall less naturally. However saline implants do have the advantages over silicone gel of less capsule contracture, smaller incisions required, and an overall reputation of greater safety. Both textured silicone and saline implants experience rippling, but in general saline implants ripple more and are more palpable, i.e. they can be felt and detected by feel more easily. Another major problem with saline implants is the leakage and deflation rate, which seems to be about 50% over a period of 10 years. In a matter of hours or days of a rupture the breast will become totally flat again.
Double Lumen Implants (Combinations of Silicone and Saline)
These implants consist of two lumens, or envelopes, one inside the other. In some models, the inner envelope is pre-filled with silicone gel, and the outer envelope is filled with saline at the time of surgery. In other models, the relationship is reversed and the inner envelope is filled with saline. Some studies suggest that the double-walled model results in a softer, more natural appearance because it reduces the incidence of capsular contracture, also the amount of saline can be adjusted at the time of surgery to the optimum fill.
Model Andreja Pejic came out as a transsexual woman in July 2014, and thereafter seemed to enjoy good breast development. However this August 2015 photograph shows that she has probably had small (perhaps 150cc) anatomically shaped breast implants.
Hydrogel Filled Implants
Technically hydrogel is composed of 92% Saline and 8% Polysaccharides, i.e. it's a mixture of salt, water and sugar. The Hydrogel implant is claimed to have the safety of standard saline implants but with all the benefits of a gel that will simulate the firmness and suppleness of natural breast tissue.
Used in many areas of medicine for such devices as replacement tendons and arterial transplants, hydrogels are believed to be safe and completely biocompatible. In fact, the majority of our body tissue is made up of naturally occurring hydrogels. In the event of leakage or rupture, the body will safely absorb the implant content.
In December 2000 the Medical Devices Agency of the United Kingdom issued a safety warning against the use of the popular Hydrogel breast implants manufactured by Poly Implant Prosthesis (PIP). The MDA's review has identified that the manufacturer's (only one brand has been used in the UK) biological safety assessment of this product in inadequate, due to the lack of long-term toxicity data or clinical follow-up, together with methodological flaws in some of the pre-clinical tests.
PVP-Hydrogel Filled Implants
The polyvinylpyrrolidone (PVP) has long been used in tablets and other medical applications and is considered biocompatible. Water-soluble, PVP-Hydrogel can be safely excreted through the kidneys in the event of traumatic rupture, it will not be metabolized by the body. The implant manufacturer suggests PVP implants have improved radiolucency over silicone gel-filled or saline-filled implants, allowing clearer visualization of the breast tissue during a mammography.
There are two styles of PVP-filled implants: pre-filled and inflatable. Like other implants, PVP-filled implants all have a textured silicone elastomer shell.
Plant Oil Filled Implants
Plant oil filled implants have developed from the concern over health safety issues relative to the silicone gel-filled implant. These breast implants filled with a natural vegetable oil promised greater safety for women. They also reportedly have more natural feel and appearance than saline implants, but little is yet known about the long-term effects or problems associated with these. They are available throughout most of the European Union but are still undergoing clinical trials in the US and Canada.
One of these new type implants, called Trilucent, contains triglyceride, an oil from soya beans that has been used for 40 years as a nutrient in intravenous feeding and as a drug carrier in injections. The manufacturers of Trilucent believe, the vegetable oil can be metabolized and excreted by the body like saline, but that it is also resistant to bacterial and fungal contamination whereas saline is not. Its lubricating properties also means that it should not rub the inside surface of the implant; this has been linked to leakage's in conventional implants. However, in June 2000 the Medical Devices Agency of the United Kingdom issued a safety warning against Trilucent breast implants because of health concerns and recommended their removal. There is no evidence of any serious medical problems but tests have shown that material produced if the oil breaks down in the body could potentially cause cancer or damage to a foetus.
Comparison
A comparison of the three most popular type of implant filling materials:
SILICON GEL
SALINE
HYDROGEL
Feel
Feels soft, natural but so called 'cohesive' is quite firm.
Feels firmer than real breast.
Feels like silicone gel, slightly firmer. At body temperature almost like breast tissue.
Preferred Insertion Route
Submammary
Periareolar most common, but transumbilical and transaxillary also possible.
Submammary and sometimes periareolar
Capsule or Hardening
Capsular contraction (hardening) frequent
Capsular contraction rare.
Capsule formation rare. To be proved by Clinical Trial.
Cost
Cost more than saline - some more than double.
Base line cost.
Same cost as saline.
Sizes
Sizes in increments
Sizes in increments but over filling is possible.
Sizes in increments
Availability
Freely available in UK. Not officially available in USA*.
Freely available.
Widely available in Europe. Limited to trial only in USA.
* Requires special approval from the Therapeutic Goods Administration on an individual patient use basis. Strict criteria on use.
Shape
Implants come in two shapes:
"Round": The majority of breast implants are of this shape.
|
"Anatomical": Some Doctors prefer a shaped implant in selected patients for a variety of reasons.
|
Round implants tend to provide more upper breast fullness while anatomical implants are contoured or tear-drop shape so they tend provide less upper breast fullness because the top of the implant is shaped and sloped more like a natural breast.
Some implants are round (below left), and some are anatomical (below right). The shape of the implants will affect the shape of the augmented breasts.
Both types of implants increase breast size. The girl can often select the type depending on the look she wants to achieve.

 Round implants tend to provide more
upper breast "roundness".
Round implants tend to provide more
upper breast "roundness".


Anatomical implants are contoured or Tear-Drop. They tend provide
less upper breast "fullness" because the top of the implant is shaped and sloped more like a natural breast.
A transwoman with the common give-away of small areola, however the appropriately sized anatomical implants make her breasts seem quite natural.
The main advantages of an anatomical implant over a round implant are:
It is not as wide as a round implant and therefore does not go out under the arm as much.
|
It is filled tighter than round implants thus maintaining the fullness in the upper parts of the breast, even in the upright position. This is made possible due to its anatomical shape.
|
Folds and ripples and wrinkles are less common than in textured round implants.
|
The overall shape is improved.
|
In some women it may improve the balance between the breasts and hips, creating an overall hip-slimming effect and a more desirable figure.
|

An exceptionally attractive transwoman with good quality breast augmentation, but the combination of small areola and round semi-spherical implants makes her breasts seem unnatural on inspection and reduces her passability as a woman.
However, many transsexual women prefer the Pamela Anderson look that can be best achieved with large round implants. Also, a recent study has [perhaps controversially] concluded that the result sought to be achieved by anatomical implants, that is, that the implant has a teardrop shape which is more natural in appearance, is achieved just as well by round implants. The study demonstrated that when a round implant is imaged within the breast in a woman who is standing, the implant takes on the same anatomical shape as the anatomical implant. The study also found that when lying down, the round implant is more natural in appearance than the anatomical because the anatomical implant retains its teardrop shape in this position whereas a round implant does not. It would seem that in at least some women, a round implants placed under the muscle can have a more natural appearance than anatomical implants, which may appear somewhat elongated in appearance in the same woman.
Surface
Almost all implant membranes (bags) are a silicone elastomer shell with rubber like characteristics. Two types of outers surface can be found on the outer surface: smooth or textured.
Textured Wall Implants
The outside of the implant is covered with a textured (rough) surface.
A persistent problem with breast implants is capsular contracture. A textured surface implant helps prevent the capsule, which naturally forms around the implant, from tightly squeezing the implant and thus making it unacceptably hard. Because of the way scar tissue forms around an implant, a textured surface is supposed to prevent scar tissue fibres from laying down uniformly in a parallel fashion and thus tightening up.
Most anatomical implants are textured because the implant is meant to have a top and a bottom (it is tear drop shaped), a textured surface on the implant causes the tissue to adhere to the implant enough to prevent its free rotation. Without the texture, the implant could "flip," leaving the implant upside down and misshapen in appearance. While this can be corrected manually or surgically, it is not an ideal happening!
One problem that causes many surgeons to avoid textured implants is the apparent increase in the chance of visible rippling compared with smooth implants. The same characteristics of the textured surface that cause the scar tissue to form irregularly around the textured implant also cause it to appear rippled in appearance. Also, due to their due to their thicker walls textured implants often have a less natural and harder feel than smooth implants, and can appear unnaturally solid.
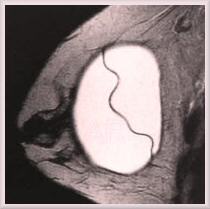
A MR scan of a round, smooth
walled, silicone gel implant in
place within a breast
Smooth Wall Implants
Smooth walled implants have an outer membrane or shell with a smooth feel.
Smooth shell implants are less likely to cause visible rippling (especially if placed below the pectoral muscle) and are more natural to the touch because they are made with thinner walls than textured, anatomical implants. Also, unlike anatomical implants, round implants do not require texture because they can rotate within the capsule and pocket without any change in appearance.
Given these advantages and some controversy over whether textured implants actually reduce the rate of contracture significantly enough to warrant the potential disadvantages, many doctors prefer to use smooth, round implants, usually placed under the muscle which is also claimed to further reduce the incidence of capsular contracture.
Comparison
A comparison of the three alternative saline-filled implant shapes and surfaces:
Anatomical Textured Saline
Round Saline Textured
Round Smooth Saline
Appears to have the most forward projection of the breast for any given volume.
Appears to have slightly less forward projection of the breast for any given volume.
Narrower breast, with least bulging out under the arm.
A little wider breast on the chest giving a round look.
In theory, less pocket creation out under the arm could pose less risk to damage to the sensory nerve to the breast.
The sensory nerve to the breast is at risk of damage as the pocket is created.
Most natural appearance with nice slope to the top of the breast.
Some bulging at the top of the breast at first and later may become somewhat concave.
Rather firm feel to the breast.
Softer feel to the breast.
Softest feel to the breast.
Occasional ripples.
Most prone to ripples.
Ripples are very rarely a problem.
Planning and placement requires extra care. It is important to prevent the implant turning around by careful pocket preparation. Texturing helps to fix the implant in position.
Requires careful surgical planning and placement, because texturing tends to fix the implant in place. It does not matter if the implant turns around, but the texturing makes this unlikely.
Standard surgical planning and placement. It does not matter if the implant turns around.
Texturing may help reduce the incidence of capsular contracture.
Capsular contracture may be slightly more likely.
Post-operative breast massage to reduce capsular contracture is not normally recommended by implant manufacturers (it can void warranty) or surgeons.
Post-operative breast massage to reduce the incidence of capsular contracture may be recommended..
Surgeons will usually recommend placing all these implants under the pectoralis major muscle (submuscular) for best results with most women.
Size
Breast implants are available in a wide variety of volumes, normally ranging from as little as 120 cc to about 850 cc, although expanders go up to 1500 cc. Some porn stars have pushed their breast size to outrageous proportions over multiple augmentations, finally using custom implants sizes of 2000 cc or more!
One study found that in a natal woman an average of 189cc of saline was needed to change the size of a breast by one bra cup size:
| Increasing an A cup to a C cup required a total of 391cc, or 196cc per cup size. |
| Increasing an A cup increasing to a D, cup required 437cc, or 145cc per cup size |
| Increasing a B cup to a D cup required a total of 448cc, or 224cc per cup. |
The A to D finding seems rather small, but the overall finding that [roughly] every 200cc of implant size equated to a one cup increase seems accurate.
Fairly successful large implants like Jennifer's are uncommon.
Although transsexual women generally prefer large implants (both in volume and breast width), unfortunately they often have insufficient existing breast tissue for adequate coverage of the desired size implant. If an unsuitably large implant is used then there will be an unnatural appearance with obvious implant give-away signs such as skin stretch marks (see below). Larger implants may also cause some pressure atrophy and thinning of muscle, subcutaneous fat and breast tissue or possibly even the ribs in the sub-muscular position.
Jaqueline started hormones at age 23. She had small (200ml) implants a few years later, which are are almost impossible to detect visually in her B cup size breasts.
With very large implants (800 cc and above), their weight and the effects of gravity cannot be ignored. Back pain is almost certain as a male type skeleton tries to deal with 2+ kg (5+ lbs) of weight added at a high and forward location, whilst the sheer weight of the implants will soon cause the breasts to sag and look far from satisfactory when not supported by a bra.
Smaller implants avoid or reduce the problems associated with implants - capsules, sagging, stretching of the breast skin, even breast cancer. For example, the smaller the implant the less likely that problems with capsule contraction will occur - relatively more breast tissue covers a small implant and it will therefore feel softer, and any distortion and firmness from capsule formation will be less noticeable.
When seeking breast augmentation, many transsexual women are faced with a conundrum as they typically have wide rib-cage and relatively little natural breast tissue even after several years on hormones. Small implants can be almost undetectable even nude, but result in breasts that are still unsatisfactorily small and excessively separated, with insufficient outside curve to match the body outline. But going for large implants means obviously augmented breasts, and an incresaed risk of complications.
This transsexual women had (top) 770cc saline submuscular implants with a periareolar incision, giving her a 36C bra cup. She had these replaced with inflatable implants filled to 1000cc (bottom), and is hoping to eventually reach 1400cc to give her a full E or EE cup.
Post-Operatively Adjustable and Expander Implants
Skin and other tissues when subjected to a gradual stretching force will not only stretch, but will also actually grow and expand.
There are now two alternative techniques that make use of this fact for breast augmentation:
1. Adjustable Implants: This method uses an adjustable saline implants that can be enlarged step-by-step after surgery by the injection of saline into it.
2. Tissue Expanders: This uses temporary tissue expanders (very similar to saline breast implants) that are later replaced by permanent long term implants.
Adjustable Implants
When relatively large implants are desired then 'inflatable' adjustable fill implants have become increasingly popular. (Adjustable implants are sometimes referred to as "Spectrum Implants", after the popular brand from Mentor Corporation)
It's uncertain that these pictures are actually of a transwoman as claimed, but they are still interesting.
Age: 28, Height: 5'1"
Implants: 425-510cc, smooth, round, Mentor Spectrum adjustable
Placement: Submuscular, inframammary incision
Bra cup size: 34A to 34D
The procedure is relatively simple. The desired breast size is discussed prior to the operation, remembering that the maximum volume of which cannot be changed after the procedure without further surgery. The surgeon then inserts - in a deflated or largely deflated state - the appropriate implants, usually under the pectoral muscle.
Breast expansion begins postoperatively after the implant has been placed. After the surgical incision has adequately healed (ordinarily about two to three weeks) the expander is gradually inflated in the surgeon's office through weekly injections of saline solution by way of a small needle placed through the skin. Over several months, the implant is slowly increased in volume by repeatedly injecting additional saline solution into the implant until the appropriate volume and symmetry is reached. For example, an implant in the range of 400 to 700 cc can be filled at the time of placement with about 120 to 300 cc, assuming the woman waits two weeks following surgery before beginning expansion and then inflates weekly with 100 cc, about seven weeks are required for full expansion.
Transwoman "Barbie" opted for adjustable implants to increase her from a hormone induced B. Over a period of a year she went from an initial D cup (left) to a G (centre), before reducing to a more natural E/F (right) when she had the valves removed.
Adjustable implants use what is known as a "remote filling port", a small button-like valve device placed beneath the skin adjacent to the expander and which is connected to the implant/expander by a small, soft tube. About 6 months after the original procedure another minor surgical procedure is performed to remove this rather noticeable device, but thus prevents any further adjustment.
A modern anatomical tissue expander with integral filling port.
Tissue Expanders
Tissue expansion-augmentation was originally developed for female breast reconstruction after a mastectomy, being intended to expand the limited remaining tissue and create a breast pocket for a long-term breast implant, but the technique also offers several advantages over standard breast augmentation methods when significant augmentation is required with little breast tissue to work with.
Tiffany Andrews, aka Holly Sweet. Her claim to be an E cup seems to be an underestimation! However the nipples are high, and as is so often the case with transgirls - the areolae are relatively small.
The procedure is initially the same as for adjustable implants. After the expander "fill" period - which may last 2-3 months - there is a settling-in and stretching period of up to six months during which no more saline is added. This second period allows time for the expander to stretch the skin and the breasts to develop a natural looking sag. To speed this process up, the expandable implants is often overfilled by between 100-150 cc compared to that needed for the target breast size. Eventually another procedure is undertaken to remove the temporary tissue expander implants and normal long-term implants (i.e. typically saline or silicone) are inserted into the pocket formed by the expanders.
Like adjustable explants, tissue expanders (or simply "expanders") used to have a filling port. However removal of this remote filling port at the time of long term implant placement is difficult and requires an additional small incision, so most modern expanders have an integral filling port that consists of a metal lined pocket within the expander itself. The surgeon precisely locates the filling port prior to each injection so that damage to the expander does not occur. Removal of these expanders is thus greatly simplified when inserting the long term implants, and no additional incisions are needed to remove the filling port.
Advantages of Adjustable's and Expander's
The technique offers several important advantages over standard breast augmentation methods when significant augmentation is required. It is increasingly favoured by transsexual women because of:
The natural final appearance of even very large breasts.
|
Many of the shape problems normally encountered with large volume implants can be overcome by the slow stretching method.
|
The stretch marks normally associated with large implants are reduced or even avoided.
|
There is normally a size limit to submuscular augmentation, if a woman with "AA to A" cup breasts wishes a significant augmentation (greater than 400 cc), then this is the method of choice. Volumes of greater than 1000 cc can be possible with this method.
|
Scar tissue from prior procedures can inhibit a good result with ordinary implants. Expander implant can overcome these problems.
|
The ability of the women to have very direct influence in the final size and shape of her breasts, without additional surgery.
|
Significant differences in the size of the two breasts can be equalised.
|




Expander implants can achieve large increases in
breast size without appearing obviously "false"
Another use of the expander is to change the shape of the breasts, either to the "scooped" look or the rounder look, depending upon the patient's preference.
The final results are often absolutely outstanding, with incredibly natural looking large breasts. Indeed, some well-known shemale's have used them to achieve outrageous breast proportions.
However, there are several disadvantages:
Only saline-filled implants can be used as adjusters, and saline implants are generally considered to have a less natural feel and sag than silicone gel or other alternative fillers. Saline expanders can later be replaced by silicone implants, but this means more surgery.
|
Every time the implant port is accessed - for injection or removal - there is a small risk of an infection.
|
Back problems are associated with very large breasts. A lot of women have at least temporary back problems, which usually but not always subside after a few weeks.
|
Once the valve of an adjustable implant is removed, the implant cannot be deflated and re-inflated as can the standard smooth round saline implant. This would be necessary if a capsule contracture were to occur, or the pocket needed to be repaired due to stretching of malposition of the implant due to problems with the pocket, e.g., the implants settling in too low, etc. They would have to be removed intact, which requires a longer incision and scar, and risks injuring the implant.
|
Another disadvantage of the adjustable/expandable procedure is that it is more expensive than other augmentation methods. This is particularly true if temporary tissue expanders are replaced by long-term implants since clearly two sets of implants are involved and two surgical procedures are performed.
Implant Incision
There are three common incision locations for inserting implants. The nipple (areola) incision is probably the most popular, followed by under the crease of the breast, and finally the the armpit. Another potential procedure is via the belly button (navel), but this has become rare due to the damage (e.g. internal bleeding) often resulting.
Periaerealor (Nipple)
Probably the most common incision method (called "periaereolar") is around the lower edge of the areola, at the junction of the dark and light skin around the nipple. Both above the muscle and submuscular implants can be done this way and the method allows good placement of the implant with consistency. This approach can only be used if the areolae are quite large, which is not the case for most transsexual women. In woman with small areolae, the method may be impossible because the incision needs to be at least 1.5 cm long, and preferably at least 2 cm long, for inserting even a relatively small implant of 200 cc volume through it. This technique is best used for relatively small implants and so many transsexual women seeking large breasts avoid this approach.
Other disadvantages of this method are visible scars on the breast itself, more traumas during surgery and longer and more painful recovery in some cases than incisions in either the navel or armpit. However the incision is relatively small and there is a natural colour change where the areola changes to breast skin which usually hides the scar well. For most patients the incision eventually becomes hardly noticeable unless they have a tendency to scar badly.
The areola approach is the only incision method that directly damages the breast tissue and is known to be more likely than to cause problems lactating and breast feeding than other methods.
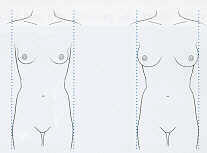
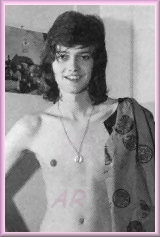
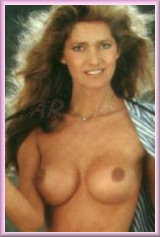
Bianca, shown:
1. Age 19, before starting oestrogen hormones
2. Age 22 after several years on hormones
3. Age 25 after reasonable quality breast augmentation using the inframammary method.
A lovely picture of transwomen Larissa Summers, only close inspection of other pictures shows the outline of the implants and the scar in the breast fold.
Inframammary (Breast fold)
Probably the second most popular incision. An incision is made above the fold of the underside of the breast. Both above the muscle (submammary) and below the muscle (submuscular) implants can be done this way and again the method allows easy access to the tissues to make a pocket to receive the implant, resulting in consistently good placement of the implant. The main disadvantage is that the scars can often be very visible when the woman is lying down topless, or even when wearing a skimpy halter-top or a bikini - the surrounding skin is all one colour which highlights the scar. The procedure is most preferable on woman whose natural breasts droop enough that the skin of the breast is touching the skin of the chest wall when standing, but this is rare in transsexual women.
Korean transsexual superstar Ha Ri-Su reveals the underarm scar of her breast augmentation. The shape and edges of her slightly over size implants are also observable.
Transaxillary (Armpit)
This technique involves an incision in each armpit (axillary) and also uses the endoscopic method of placement. This method is used primarily for those who don’t want scars on the breast and who don’t wish to have the surgery done through the navel. It has the disadvantage of being distant from the operative site, possibly making it difficult to visualize the site and control bleeding.
While axillary scars usually can't be seen, there are nevertheless small and sometimes thickened scars in the armpits which may be quite noticeable when the arms are raised while wearing sleeveless clothing. Studies have also shown that there is apparently a higher possibility of permanent loss of feeling in the nipples than other incision methods, and the method can also interfere with the nerves near the arm, resulting in numbness in the arms occurring temporarily or permanently.
Transumbilical (Navel)
The Trans Umbilical Breast Augmentation technique (usually abbreviated to TUBA or "transumbilical") provides insertion of breast implants through a small incision made in the belly button.
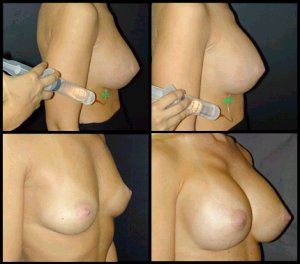
The procedure is illustrated below:


1. The breast prior to surgery.
2. A small incision is made in the navel. Through the incision, a slender instrument passes under the skin to a location underneath the breast and (in this example) pectoralis major muscle.
3. A tissue expander is inserted and placed under the breast. With the expander, a space is developed to create a pocket for the implant size requested.



4. Positioning & shape of the implant pocket is checked with an endoscopic fibre optic camera.
5. The breast implant is inserted into position uninflated.
6. The breast implant is inflated with saline. The incision is closed with a few absorbable stitches.
Insertion through the umbilicus makes it hard to position the implant accurately, generally allows placement only above the muscle, and also puts significant stress on the implant. Surgeons are not able to get as consistently good results this way as if they were working through an incision right on the breast. Because of difficulties in placement of the implant, the transumbilical method really only makes sense if there is not already a scar on the breast. Also the method cannot be used for large implants or pre-filled implants (e.g. silicone gel type).
However, this method eliminates any scarring in the area of the breast (although unsightly scaring in the abdominal area can occur instead) and recovery can be much shorter this way because there are no stitches near the arms and breast and less healing of scars and internal tissue that would be cut to pass through the areola or inframammary area. Perhaps the main risk is having to make a normal (i.e. periarealor or inframmary) breast incision if the placement did not work out during surgery, however it can be argued that that the possibility of having no scars at all was worth the try.
 Submuscular, periareolar, 600cc implants
Submuscular, periareolar, 600cc implants
Selecting the Right Incision Method
As can be seen above, each incision method has advantages and disadvantages.
If the natural breast is small and perky (relatively common in transsexual women) the underarm transaxillary approach is often the optimum approach. It involves no incision on the breast, does not interfere with the breast tissue and can achieve a perfectly symmetrical result with only minimal and well concealed scarring - unless the woman is a dancer or for some other reason often has her arms in the air with the axillae exposed frequently. If you have had no previous breast augmentation surgery and avoiding any visible scars is very important, then the navel (transumbilical) method is an option, but it has the least consistent record as regards good placement of the implants and should only be done by surgeons who specialised in this technique. For women who have large areolae (relatively rare in transsexual women) the periaerolar incision is an attractive option which allows reliable implant placement, it can be used with any type and size of implant and is very versatile, allowing shaping of the breast tissue and muscle to form a natural shape around the implant. The incision made in the wrinkles of the brown skin round the areola generally heals with the only slightly visible scaring and is thus very popular. Finally, the inframammary incision allows good placement but leaves the most visible scaring except with pendulous breasts, it's best reserved for large and very large pre-filled implants.
In general the surgeon will make every effort to ensure that the incision (typically varying from 2 cm long for small unfilled saline implants to over 5 cm for large pre-filled silicone gel implants) is placed so that the resulting scars will be as inconspicuous as possible, given the women's circumstances and priorities. A big potential advantage of saline implants over silicone gel implants is small and well hidden scars - saline implants are usually filled after insertion so the incisions will be just 2-3 cm in most cases, and insertion techniques such as the transumbilical method can inconspicuously locate these small scars if desired.
At least 90 percent of all incisions, if properly closed, will result in an inconspicuous scar after maturation is complete - but unfortunately patients do differ in their healing characteristics and a very few may scar badly, and the possible scaring should be considered when selecting the implant method. E.g. If an ability to topless sunbath without showing off implant scars is important, then small implants via the transaxillary method may well be preferred over larger implants via the inframammary technique.
Breast Implant Placement
Chest Wall Anatomy and the relationship to Breast Implant Placement
The final outcome and shape of breasts after implant enlargement or Augmentation Mammaplasty is in large part determined by the relationship of the implants to the pectoralis muscles of the chest wall. Implants can either be placed above (over) the pectoral muscles, or beneath (under) the muscles. Both techniques have advantages and disadvantages. Furthermore, the route of placement of implants under the muscle also determines whether the implant is totally covered or only partially covered by muscle when it is placed in the sub-pectoral plane. A number of consequences may result according to the position and route of placement of implants, and some of the potential complication risks of Breast Augmentation can thus be altered by adhering to certain principles of implant placement when feasible. These include limiting risk of capsule contracture, limiting the "round" look of implants, preventing visible rippling or wrinkling of the implants, preventing "bottoming out" of the implants, and most importantly, limiting compromise of Mammography after augmentation.
 Exceptionally good result given the minimal amount of natural breast development.
Exceptionally good result given the minimal amount of natural breast development.
Subglandular (above the muscle)
This means placement of the implant above the pectoral muscles but below the mammary gland. Technically, all implants are subglandular because implants placed below muscle are also below the mammary gland. However, this term refers to placement just below the mammary glands and above the muscle. This placement is also referred to as retroglandular or submammary.
While many surgeons prefer this method when using silicone gel implants, if saline implants are used then in many cases the results are suboptimal. This is because saline is water, and does not feel as much like breast tissue as silicone.
If the breast tissue, skin, and subcutaneous tissue are too thin, one can see the outline of the implant, actually feel the implant edges, and often see rippling in the skin. In these cases, it would be better to place the implant under the muscle.

The diagrams to the left show implant placement over the muscle in the sub-glandular position.
In the "over" approach the implants are inside the breast, completely in contact with the breast tissue, above the muscle. It provides a round augmented look, which is less natural but is preferred by many women.
Advantages of the technique are ease of the surgery, avoidance of a breast lift (mastopexy) for mild sagging or drooping (ptosis) of the breast, less post-op discomfort since only skin and fat are cut. The approach also allows insertion of oversize implants.
Disadvantages are marked interference with mammograms, clear visibility and feel of implant edges, visible and palpable rippling of the skin over the implants, especially with any textured implants, higher rate of capsule contracture, high rate of later implant downward migration or "bottoming-out", and difficulty correcting later ptosis problems when they occur. Saline implants over the muscle are avoided if possible.
Subpectoral (partial submuscular)
Although often included with "submuscular" placement (see below), subpectoral means placement of the implant below the pectoralis major muscle. In subpectoral placement, the implant is only partially submuscular due to the nature of the pectoral muscle under which the implant is placed. The lower half of the implant is not covered by muscle in this type of placement. This placement is also referred to as retropectoral.

Partial submuscular implant coverage with implants placed under the muscle, usually via a periareola incision or an inframammary crease incision.
This placement causes disruption to the muscle support fascia at the lower pole of the implant in order to allow the implants to enter the space under the muscle.
With this approach the implants are mostly behind the breast.
 Genetic woman. 34A to 34C
Genetic woman. 34A to 34C
Moderate degree of tubular breast treated with smooth round 475cc subpectoral implants. Note the natural roundness to the base and bottom of the breast.
Advantages include mostly separating the implants from the muscle, facilitating unobstructed mammography, a more natural look with a soft transition from the flat of the upper chest wall to the round shape of the implant, much less visibility and feel of the implant edges, usually no rippling (except textured implants), and low risk of capsule contracture, as long as the implants have not been contaminated by ductal germs while being passed through the breast tissues.
Disadvantages include a bit more discomfort early post-op, technique a bit more difficult than over the muscle, and the loss of the lower pole support fascia which leave the implants supported by the same weak skin tissues as implants over the muscle, leading to later downward bottoming-out of the implants in a few patients as is frequently seen in implants over the muscle.
Submuscular (under the muscle)
Although many refer to subpectoral placement as "submuscular," fully submuscular placement actually means placing the implant under not only the pectoralis major muscle (covering the upper portion of the implant) but also under related muscles at the lower half of the implant. Because of the thickness of the muscle, the problems stated above can be improved with this technique, but it, too, has limitations, the most important being that the implant size is limited to between 300 to 400cc’s, which may be insufficient for some transsexual women.

A complete submuscular implant. The support fascia is an extension of the muscle envelope from the pectoralis muscles to the abdominal rectus muscles, and the finger shaped serratus anterior muscles to the sides. This stout collagen sheet slowly stretches after implant placement and provides reliable long-term internal bra-like support to prevent "bottoming-out". Complete muscle coverage of the implant, without cutting through the muscles, can only be achieved by transaxillary approach, entering the space under the muscle where it lies closest to the skin in the anterior axillary fold.
The advantages of this approach are ease of placement, natural breast shape no implant visibility, no rippling of the implant surface (except textured implants in thin women), lower capsule contracture risk, since the breasts are completely separated from the implant, and no ducts with germs are damaged while placing the implants, low mammography interference, good internal support, and no scars on the breast.
Disadvantages are the difficulty mastering the procedure, muscle discomfort post-op, and implants which tend early to be a bit full superiorly, until the support fascia stretches.
Advantages and Disadvantages:
Capsular contracture - Many surgeons believe, based upon clinical studies regarding placement of the implant and contracture rates, that placing the implant below the pectoralis muscle (subpectoral) or fully submuscular, reduces the rate of capsular contracture when compared to above the muscle placement of the implant. Keep in mind that there is not total agreement as to whether this is truly the case. One alternative that has been suggested to prevent capsular contracture is the textured implant which, even if placed above the muscle, is also supposed to reduce the rate of capsular contracture. Whether this is true is also the subject of some debate. Furthermore, many believe that textured implants are more likely to create visible rippling. Surgeons who disagree with this view of textured implants claim that rippling is a result of improper filling of the implant and not at all with the surface of the implants.
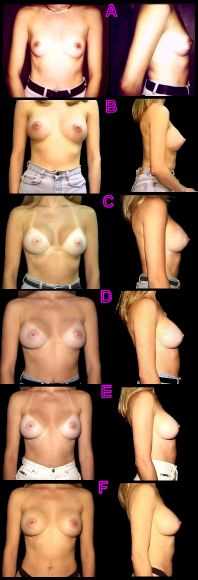
(Left) A series of photo's showing how implants settle over time. This 33 year old woman had 375cc implants via a transaxillary incision, going from a 36C to 36D cup size.
A. Pre-op
B. 8 Days post-op - Note upper pole breast fullness and slight irregularity of the lower breast pole contour due to tightness of the fascia (muscle envelope) and the overlying skin.
C. 3 Months post-op - Breasts are still overly round, particularly in the side view, but superior fullness is subsiding and the lower pole is relaxing.
D. 6 months post-op
E. 1 Year Post-op - Upper breast pole now has a natural slope, and the lower breast pole has developed a normal soft curving contour.
F. 2 year post op
Rippling - in women with little breast tissue, subpectoral or fully submuscular placement is likely to reduce the chances of visible rippling of the implant. This should be true regardless of the originating reason for the rippling (underfilling or textured surface, depending on the opinion held) because the implant is partially or fully covered by muscle, in addition to breast tissue.
Mammography - although technology increasingly makes better breast imaging possible with and without implants, placement of the implant below the muscle is thought generally to improve mammography by making it less likely that the implant will prevent proper imaging of all of the breast tissue. Subglandular (or above muscle) placement, on the other hand, is thought to be more likely to interfere with imaging. While implants containing alternative fills such as soy or peanut oil have been experimented with due to their being radiolucent (they allow imaging to pass through the implant), none have been approved for use so the above muscle placement of the implant still causes some concern with regard to mammography.

Premature breast implants, inadequately covered by hormone induced breast tissue, is a common problem.
Appearance - Initially, and especially with silicone implants, implants were predominantly placed above the muscle (subglandular).
Most surgeons agree that where:
(i) the woman has adequate breast tissue to disguise the implant, and
(ii) there is no unfortunate rippling or contracture, then above the muscle placement results in the most natural looking result because the implant is behind only the tissue itself, and the tissue that is being augmented takes on the augmented shape. It is also preferable for women who work out their upper body a lot as their muscles can contract implants that are behind the muscle into a distorted shape with an unusual appearance.
However, for women with little to average breast tissue - which includes most transsexual women - under the muscle placement can help to avoid the "fake" look of implants that are apparent because they are closer to the surface.

Leslie, transwoman star of the now cult 1978 'B' movie "Let Me Die A Woman". A hyper-critical examination of her initially very natural looking breasts shows that the implants have sagged, although they remain within the breast tissue.
Sagging - For fully submuscular placements, and to a degree subpectoral placement as well, the implant is better supported than in subglandular (above muscle) placement, resulting in less sagging (ptosis) of the augmented breast in the long term.
However, if a woman already has substantial breast tissue then a submuscular or subpectoral placement can be a problem because the pectoralis muscle tends not to sag. But placement of the implant behind the muscle means that the implant is likely in high on the chest. The passage of time can result in the sagging of the existing breast tissue, which increasingly looks like separate tissue hanging from the firmer, higher mound of the implant. A mastopexy (breast lift) can become necessary to restore the appearance.
Due most of the factors listed above, most surgeons prefer under the muscle placement, whether subpectoral or fully submuscular, but again, the patient's physical characteristics will affect the decision as well as the surgeon's preference.
Comparison of various implant positions:
Issue
Implant Location
Over Muscle
Partial Under Muscle
Complete Under Muscle
Mammography
Marked interference even with Eklund distraction technique
Minimal interference with Eklund distraction technique
Minimal interference with Eklund distraction technique
Capsule Contracture
Highest risk
Lower risk
Lowest risk
Rippling
Highest risk especially with any textured implants
Lowest risk even with textured implants
Lowest risk even with textured implants
Natural Appearance
Less Likely (but not desired by all patients)
Likely
Likely
Implant Bottoming out
Frequently seen - leads to inframammary scars riding up onto the breast
Frequently seen - leads to inframammary scars riding up onto the breast
Rarely seen
Use in presence of borderline sag
May correct sag in short term, but usually requires later ptosis repair because breast support ligaments (of Cooper) are cut
May correct borderline sag but may require immediate or later mastopexy (breast lift)
May correct borderline sag by pectoral sweep manoeuvre, but may require immediate or later mastopexy
Late Sag requiring repair
Frequently seen especially if over muscle was done to try to "fix" sag
Less frequent
Less frequent
After Surgery

This transsexual woman had relatively large breast implants placed above the muscle (subglandular) at age 19 (top). Just five years later gravity had caused "sagging boobs" (bottom), with the shape of the implants still obvious.
During the first 24 to 48 hours after your surgery, you will experience the most discomfort. Your breasts will be swollen and very tender. Although every woman's recovery time is different, you should be able to resume many of your regular activities after about one week. You will need to wait at least one month before resuming any strenuous activities.
Should any problems occur after surgery, contact your doctor immediately. This is especially important if your temperature is elevated, or one of your breasts is noticeably more swollen and tender to the touch, painful, red or inflamed.
After surgery, implants will ride high on the chest. It will normally take 4-12 weeks for them to "drop" into place. The more natural breast tissue you have and the smaller the implant, the more natural the look. Keep in mind, most women wish they had gone larger! Placing them under the muscle also allows for a more natural appearance. As you age, your natural breast tissue will sag, the implant will not.
Risks and Problems
The implant manufacturer Mentor Corporation conducted clinical testing of its saline-filled breast implants to determine the most common short-term risks associated with their implants. The Saline Prospective Study (SPS) was a 3-year study to assess all complications with breast implants as well as patient satisfaction, body image, and self-concept. Patients were followed annually and data through 3 years are available. The SPS enrolled 1,264 augmentation patients, 76% of which returned for their 3-year visit. The results are tabulated as follows:


Disappointing breast augmentation's for the TS girls Kelly and Keri (above), but Camila (below) is happy to show off a better result.

Augmentation Complications
3-Year Risk Rate
By Patient
N=1264
By Implant
N=2526
Wrinkling
21%
20%
Reoperation
13%
10%
Loss of Nipple Sensation
10%
8%
Capsular Contracture Grade 3/4, or grade unknown
9%
7%
Implant Removal
8%
6%
Asymmetry
7%
5%
Intense Nipple Sensation
5%
4%
Breast Pain
5%
4%
Leakage/Deflation
3%
2%
Implant Palpability
2%
2%
Infection
2%
1%
Breast Sagging
2%
1%
Scarring Complications
2%
2%
It's worth noting that more than 1 in 5 (21%) women experienced problems with wrinkling and ripples, and probably more than half experienced some form of problem, of greater or lesser significance, within 3 years of their breast augmentation. Clearly breast augmentation is still not a trouble free experience for many women, whatever some surgeons may try to imply.

Poor quality breast implants are the bane of many attractive transwomen. Of course the cost of using a top surgeon is often the reason.
Satisfaction
Over half of all transsexual women eventually have breast augmentation and the results are well documented. Its informative to quote the results of one survey here to see if the pain, expense and complications are all considered worth it by transsexual women.
One hundred and seven post-operative male-to-female transsexual woman were surveyed an average 5.5 years after mammaplasty (range, 16 months-17 years. The age of the woman ranged from 22 to 76 years (average, 41 years). Seventeen of the 107 women had undergone further augmentation mammaplasty, on average 57 months after the initial mammaplasty. The average size of implanted prostheses was 258 ml (range, 130- 450 ml).
Eighty women (75%) indicated satisfaction with the final outcome of the mammaplasty. The median postoperative cup size in this group was B (range of postoperative bra size, 30B-40D).
The remaining 27 women (25%) were unhappy with the results of mammaplasty. The median postoperative cup size in the 18 women who still felt their breasts to be too small was also B (range of bra size, 30B-48E). The average size of current prostheses in these 18 women was 261 ml.
 A good result using the periareolar method
A good result using the periareolar method
It's notable that despite the desire of many transsexual women for large breasts, the two women with an augmented 40D and 48E bra size are clearly exceptional. The most common result is a moderate B cup and the average implant size is an also moderate 260ml, the largest being only 450ml. This, and the relatively high percentage of women feeling that their breasts were still too small, is unfortunately an indication of the limitations imposed on augmentation by the small natural breasts typical of pre-augmentation transsexual women. See the at the bottom of this page photo of an augmentation by the famous surgeon Dr. Douglas Ousterhout as a demonstration that even the best surgeon can only achieve so much with the material they have to work with.
Common Implant Problems
Capsular Contracture
When any type of breast implant is inserted, the body's immune system reacts by forming a protective lining made from collagen around it to protect itself from this foreign body. This is referred to as the "capsule" or "tissue capsule."
The formation of a capsule is normal and happens in everyone regardless of whether the implant is smooth or textured, silicone or saline. Under ideal circumstances, the capsule maintains its original dimensions and the implant rests inside it, remaining soft and natural appearing. However, for reasons that are unknown, in some women the capsule has a tendency to shrink, squeezing the implant. An implant that is compressed hardens like a balloon, i.e. the tighter the capsule becomes the firmer the breast feels. This problem is called "Spherical Capsular Contracture". It has been known since the very early days of implants and has always been considered to be the main problem with breast implants.

Transwoman can seek very different appearances after breast augmentation surgery.
The degree of capsular contracture is measured on the "Baker Scale", from grade 1 to 4. Grade 1 means the breast looks and feels so soft that the capsule is virtually undetectable; while Grade 4 means the implant is painful and as firm as a grapefruit, and that it is being distorted in shape and squeezed out of position.
No matter the degree of capsular contracture, it is not the implant that gets hard, if the implant is removed it is as soft as when it was inserted, it is the interaction of the capsule with the implant that makes the breast feel firm. Capsular contracture alone does not cause implant rupture because the force is exerted evenly around the surface of the implant.
Encapsulation may occur immediately after surgery or many years later, and may occur on one or on both sides. The incidence of capsular contracture approached 100% in the 1970s, subsequent modifications in implant design and the surgical procedure have reduced this undesirable effect significantly, according to various studies and surgeons claims, the frequency of significant encapsulation (Grade 3 or 4) among women with saline-filled breast implants currently ranges anywhere from 5 to 18%.
It should be noted that a mild to moderate degree of contraction usually. Most encapsulation is of a mild degree (Grade 1 or 2) that doesn't detract from the quality of the augmentation result and is not considered clinically significant. Indeed, for some women a mild degree of firmness in their breasts, similar to a pubescent girl's, may actually represent a desirable outcome.
The treatment of severe capsular contracture is usually surgical. In an "open capsulectomy" the surgeon scores, or cuts, the capsule to release its hold on the implant. In a "closed capsulectomy," the entire capsule is surgically removed. The body then forms a new capsule but the hope is that it does not contract as the old one did. Capsulectomy is a more extensive operation than capsulotomy but has a higher rate of success in correcting contracture. Only a relatively small percentage of women with implants develop capsular contracture severe enough to require surgical treatment. The rare patient develops repeated capsular contracture but in the majority of cases it can be successfully treated.
Implant Wrinkling and Breast Rippling
Some transsexual women insist on choosing excessively large and inappropriately shaped implants for their available breast tissue coverage in an unrealistic desire to achieve "Playboy" breasts. At best its very obvious that they've had breast implants, whilst in the very worst cases the implant can actually start to emerge through a hole in the skin at the bottom of the breast.
The most common visible problem with overly large breast implants is traction rippling. Rippling looks like someone had their fingers on the breast and left indentations, it is not a permanent rippling in most cases but a ripple occasionally as the implant moves and literally ripples, giving the skin a wave-like appearance instead of the smoothness you see in a normal breast. When you spot an actresses or lingerie model with obvious and over large implants, then you have probably seen this phenomenon. Some 20% of genetic women with implants experience problems with rippling, and the incidence is probably even higher in transsexual women who tend to over size their implants.

Age: 30, Height: 5'5", Weight: 115 lbs
Implants: 700cc filled to 780cc, textured, saline
Placement: Submuscular, with periareolar incision
(Above) An example of severe implant malposition, drop-out of the inframammary creases, severe bottoming out, and obvious traction wrinkling. The problems are all due to much too large a size implant, with a textured shell, in a woman with little body fat (i.e. thin!) and inadequate soft breast tissue coverage.
Every breast implant has at least a little bit of wrinkling, an irregularity of its surface. Some implants have very little, and some have a lot of it; if there is little, then it may not even be detectable. If there is more, it may be felt, and if there is a lot of wrinkling, then it can be felt and even seen as rippling. In general, the degree of wrinkling depends upon several factors that work to either hide or reveal wrinkling or rippling. The areas where rippling is usually most apparent are the outer side near the arm, along the bottom, and towards the cleavage, in that order. The rippling is most objectionable when it is visible at the top of the breast. For that reason, placing implants beneath the large pectoral muscle can be particularly advantageous with saline implants. The thickness of the muscle obscures whatever wrinkling there might be, in the same way that a thick carpet will hide uneven floor boards.

Age: 40, Height: 5'7 ", Weight: 110 lbs
Implants: 370cc, smooth, saline
Bra Cup Size: 36 C
Note: Implant displacement and severe bottoming-out, again caused by overlarge implants for a thin woman with minimal natural breast tissue.
Saline implants tend to ripple more than silicone gel or other materials. It is in the nature of saline inflatable implants to have wrinkling of the shell. This is because the shell needs to be thick and strong enough to last as long as possible, and because the saline (salt water) fill shifts with changes in body position. In addition, if a saline implant is not filled up to the optimum, which may require overfill, there can be rippling at the top of the breast also. Every saline implant has an optimum volume of saline fill, a volume that gives the best balance between either wrinkling (caused by not enough saline) or too firm/round (caused by too much saline). The difference between inadequate volume and the optimum volume is astonishingly small, around 10%, which may be only a couple tablespoons of water! Women who are troubled with rippling because their implants were not filled to the ideal optimal volume may need an operation to add that critical tablespoonful of saltwater that makes all the difference.

These transsexual women demonstrate a look all too common - solid, unnatural, widely spaced, semi-spherical breasts stuck on to the chest. This occurs when over-large implants are inserted under a minimal amount of natural breast tissue, often prematurely, i.e. before maximum possible amount of hormone induced development.

Implant Give-Away's
The Look
Despite the every effort of implant manufacturer's and surgeons, the look and feel of breasts with implants will be different (to some degree) from that of similar size real breasts. Have you ever paged through a lingerie catalogue and been sure that one of the models had breast implants? Well, that's probably because implants can make the breast look unnaturally rounded. Most implants are half spheres in appearance while natural breast shapes are more parabolic or U-shaped. Women with large implants may also get a "double breast." This is because the normal breast hangs, but the implants stick straight out from the chest wall. This makes the breast look like it has a hump in the middle when looking at it from the side. When pushed up, the implants' upper border will show through the skin. Two deeply curved upside down lines get etched in the skin. When pushed together, well... they don't push together. It is like putting too balls together; they meet in the middle and leave a gap on either side. This is in contrast to the straight line formed by natural breasts. When left alone, implants leave a flat valley-like gap where the breastbone (the sternum) is, between the implants. Natural breasts slope more gradually towards the centre.
Measure's can be taken to minimize and reduce all these problems, but they cannot be completely eliminated with the current breast augmentation technology.

The Feel
When doctors say that implants feel the same as normal breasts, they are talking about how they feel to others touching the breasts, not about how they feel to the woman with the implants. Implants can make it harder to sleep on your stomach and they often feel cold. Silicone gel and plant oil-filled breasts have a good reputation for feeling comfortable and natural to the woman, but saline-filled implants don't have the same density as tissue so the weight of the breast feels odd for its size.
The body forms capsule tissue around the implants, in some women this causes the breasts to feel artificially firm or even hard.
The difference in the feel of the breasts can also have an impact on cancer screening. If the augmented breast does not feel the same as the natural breast, it can be difficult to determine if there is a change in the breast that should be checked out. Also, there are changes that will occur in the breast due to the implant that will have nothing to do with cancer, but these changes can cause alarm when they are first noticed.
Summary

Give-away's caused by over-large implants or other factors (including poor quality surgery) include:
| Ridges - Depending on the implant size and the amount of natural tissue, the top ridge of the implant may plainly show |
| Bottoming - Bottom of edge of implant shows |
| Artificially round looking breasts, although this may be desired by many women |
| Double breast (hump in breast) |
| Excessive upward projection |
| Poor positioning of the breasts (usually too high) |
| Strange and unnatural looking nipple placement |
| Ripples in the skin - Rippling comes from not having enough natural tissue to cover the implant or having a large implant. |
| An unnaturally solid breast, with little mobility or "flop" |
| Long and very visible scars |
| Stretch Marks - May appear and are more likely with larger implants. |


Implants after little or no hormone therapy. With no natural breast tissue, only a thin layer of skin is covering the implant.
Factors that increase implant give-aways:
| Thinner woman with thinner fat layer |
| Smaller pre-operative breast size |
| Textured-surface implants (increases degree of "traction rippling") |
| Saline rather than silicone gel fill |
| Inadequate volume of saline inside saline implant |
Factors that decrease implant give-aways:
| Maximise all possible hormone induced natural breast |
development before any augmentation - a minimum of
two years hormone use is recommended
| Heavier patients with thicker fat layer |
| Larger pre-operative breast size |
| Silicone rather than saline fill |
| Optimum volume of saline inside |
Transsexual women who "pass" successfully have usually taken the advice of their surgeon and settled for appropriately shaped small-to-medium implants which give them natural appearing augmented breasts of perfectly adequate size for their build.
Breast Augmentation Examples
Non-transsexual Women
I attempt to show here a diverse range of implant results illustrative to the diverse range of procedures and implants types possible.


Age: 20
Implants: 475cc, smooth, round
Placement: Submuscular
Bra cup size: ?
Age: 19
Implants: 275 cc, smooth
Placement: Submuscular, transaxillary incision
Bra cup size: 32A to full 32B


Age: 25
Implants: 350 cc, smooth, saline
Placement: Submuscular, transaxillary incission
Bra cup size: AA to C
Age: 29
Implants: 250 cc
Incision: Inframammary
Bra cup size: 34A to 34 C/D

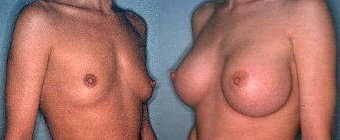
Age: 19, Height: 5'7", Weight: 115 lbs.
Implants: 300 cc, anatomic
Incision: Transaxillary
Bra cup size: ?
Age: 25
Implants: 530 cc, round, saline
Placement: Submuscular, inframammary incision
Bra cup size: A to large C


Age: 24
Implants: 395 cc, smooth, round, saline
Placement: Submuscular, periareolar incision
Bra cup size: 34A to 34C
Age: 26, Height 5'4", Weight: 107 lbs.
Implants: 430 and 440 cc, smooth, round, Mentor Spectrum expandable
Placement: Submusclar, TUBA incision
Bra cup size: 34A/B, Post 34 D


Age: 19
Implants: 320 cc
Incision: Transaxillary
Bra cup size: 32A to 34 D
Age: 19
Implants: 285 cc, smooth, round, saline
Placement: Subgandular, inframammary incision
Bra cup size: 32A to 34 C


Age: 24, Height: 5'5", Weight: 128 lbs.
Implants: 475 cc, round, smooth, saline
Placement: Subglandular, inframammary incision
Bra cup size: 32 AA to 36 D
Age: 29, Height: 5'3", Weight: 118
Implants: 570cc, smooth, round, Mentor Spectrum
Placement: Submuscular
Bra cup size: 34-36B to 34-36D


Age: ?
Implants: 700 cc, silicone gel
Placement: Submuscular
Bra cup size: ?
Age: ?
Implants: 475 cc, round, smooth, saline
Placement: Submuscular, periareolar incision
Bra cup size: ?

Age: 28
Implants: 350 ml round silicone gel implants (Mentor plus profile)
Placement: Submuscular
Bra cup size: ?
Hundreds more fully documented examples of breast augmentation, including "Before and After Photos" and a lot of other useful information, can be found at the "All about Breast Augmentation and Breast Implants Resource" and Nicole's huge "Breast Augmentation & Breast Implants Information Web".
Transsexual Women
The pictures below of Leah show one of the most successful breast augmentations that I have seen in a transwoman. The left picture was taken soon after her breast augmentation in her late 30's. This involved a inframammary incision and the skin of breast is still very stretched and the outline of the profiled implants fairly clear. The right hand picture is taken several years later and the breasts have settled in to a very natural looking appearance, probably aided by some additional hormone induced tissue development. The exceptionally large areolae are marred slightly by the surrounding area having a slight skin rash (just visible in the photo), possibly caused by the implants being relatively near to the surface.

The following pictures show Larisa. An initially good impression (left) of her breast augmentation is countered (right) by the implants being obvious and very unnatural in appearance when topless.

The following photographs are "before and after" examples of male-to-female transsexual women who have undergone breast augmentation. No details of the surgery are known except as given.

 27 years old
27 years old
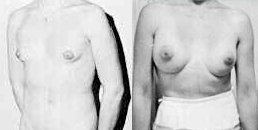

The following photographs are of transsexual women after breast augmentation. Unfortunately no "before" photo's are unavailable. Any available details of the surgery are given.

Surgeon: Dr. Douglas Ousterhout
Implants: 350cc, saline
Placement: Submuscular, periareolar incisions
Note: Notice the considerable distance between the breasts even with a high quality augmentation from a top surgeon

Surgeon: Dr Toby Meltzer
Implants: Saline, size unknown
Incision: Submuscular, periareolar incision



Copyright (c) 2002-13, Annie Richards